


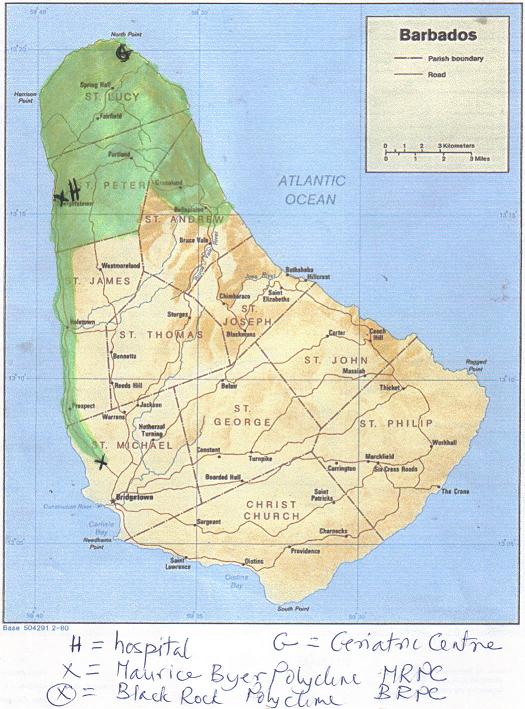
Map displays the current (or possible) available health facilities for the people of the North. These include St Joseph hospital- now allowed to be destroyed by the BLP. The Geriatric Hospital at River Bay area – to be upgraded to a Geriatric center with Physiotherapy, Occupational Therapists etc etc.The Maurice Byer Polyclinic. The Black Rock Polyclinic- which is more easily accessed than the Maurice Byer Polyclinic to those who are challenged in an ambulatory way.The St Andrew folk have as Warrens Polyclinic as an alternative
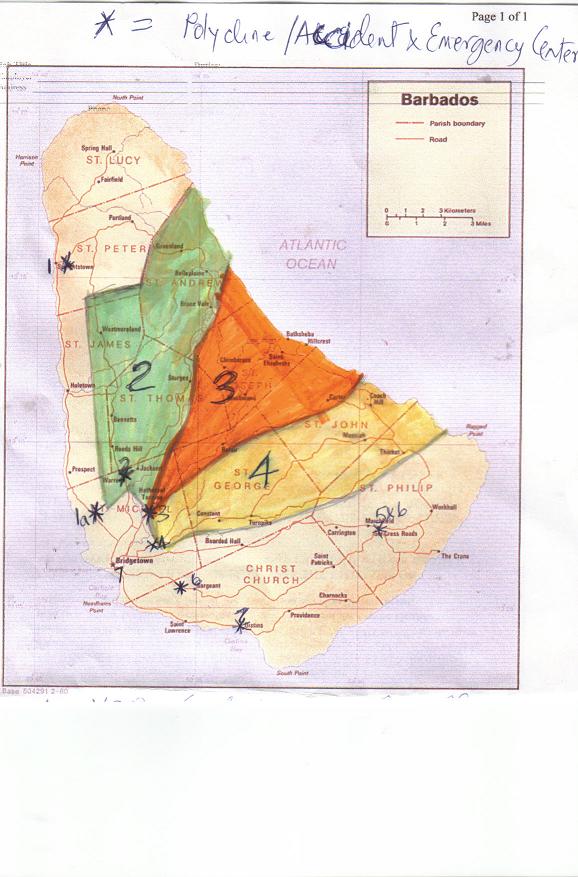
A- my proposed catchment area for Warrens Polyclinic (area 2) in green. B- my proposed catchment area for a Clinic at Hothersal Turning (area 3) in orange. C- my proposed catchment area for a Clinic on Highway 4 below the junction of Highway 4 and Highway X. I have noted in any detail the catchment areas for areas 5, 6 & 7. My “areas” are of course related to our 7 major highways. The numbers 7 on the map refer to the existing clinics on/off highway 7, ie Oistins Clinic and Sir Winston Scott Polyclinic The number 6 refers to Edgar Cochrane Clinic. The designation 5/6 refers to Six Roads Clinic.
Submitted by BU Commenter: Georgie Porgie
The new St. John Polyclinic will be completed as a matter of priority and other capital investments, both private and public, in the health care sector will be undertaken to ensure the restoration of Barbados place as a number one community health care provider, he noted.
I read the above nonsense in today’s advocate, and wonder why one would follow such an idea. Any clinic to serve the interests of the St John folk is best sited below Salters intersection where Highways X and 4 meet. By placing the clinic at this location we enlarge its catchment area, because the catchment area for such a clinic will then be most of St George, most of St John, sections of northern St Philip and an area in the central easterly section of St Michael.
We need to stop thinking parochially and in terms of constituencies, and think in terms of regions served by available public transport. To place a clinic in St John where the abandoned clinic is sited is out of the way for most St John residents using the current bus system. Currently there is a badly sited clinic at the Glebe and there was one at Gall Hill. Both of these satellite clinics Satellite clinics at these sites were established in the fifties by the late Prof Standard. But now these clinics should be amalgamated and cited below Salters intersection where Highways X and 4 meet, and where they really belong. Such a move facilitates attendance by those who depend on the public transport services in the central easterly section of St Michael.
Relocation of these clinics will also free up the building at the Glebe, and the abandoned building in St John for use as a center for educational, social and other activities (police station, courts etc, library post office, as at Holetown. By placing the Zone four Polyclinic/Emergency Center below below Salters intersection where Highways X and 4 meet, we enlarge its catchment area, and get more bang for our buck! We also free up the building at the Glebe, and the abandoned building in St John for use as a center for educational, social and other activities.
Finally the clinic does not have to be a sprawling monstrosity as some of those currently existing, in which there is a lot of unused space.


The blogmaster invites you to join the discussion.